Low-FODMAP Diet: Phases and Reintroduction
How to apply the three phases of the Low-FODMAP diet, when it may be useful in SIBO, and how to keep it from becoming more restrictive than necessary.
Editorial standards for this guide
Editorial lead
Beiker Guillen
Published
Last updated
Last editorial review
This content is for educational purposes. It summarizes public evidence, explains it in plain English, and avoids closed recommendations when the literature is uncertain or depends on clinical context.
You can review how we select sources, how we update older pieces, and the editorial limits we follow in our editorial methodology .

Quick Summary (TL;DR)
- What is it?: a temporary nutritional strategy to reduce the load of fermentable carbohydrates and observe whether symptoms improve.
- The most important thing: it is not meant to be followed strictly over the long term; it needs phases and reintroduction.
- What you’ll take away: how the phases work, what mistakes to avoid, and why personalization matters more than a rigid food list.
💡 What is the low-FODMAP diet?
The low-FODMAP diet is a temporary protocol of reducing and later reintroducing fermentable carbohydrates. It is used to explore whether certain food groups worsen digestive symptoms, and it should not stay in a restrictive phase indefinitely.
Low-FODMAP Diet: Phases and Reintroduction
The Low-FODMAP diet is a therapeutic tool that can help reduce digestive symptoms in some people with SIBO, IBS, and other functional conditions [1][2]. This guide summarizes how to apply its three phases with more judgment and less unnecessary rigidity.
Author’s note: The low-FODMAP diet is probably the topic I get the most questions about. Understanding it requires patience because it has phases, exceptions, and nuances that can’t be summed up in a single rule. I tried to organize this guide so you can consult each phase separately without having to read everything at once.
⚠️ Important: This diet must be supervised by a health professional (a gastroenterologist or a specialized dietitian). Do not attempt to follow this diet without professional supervision, as it can cause nutritional deficiencies if it is not managed correctly.
In this guide: you’ll find a clear explanation of the three phases, when it can help, what mistakes tend to make it too restrictive, and how to fit it into a broader strategy.
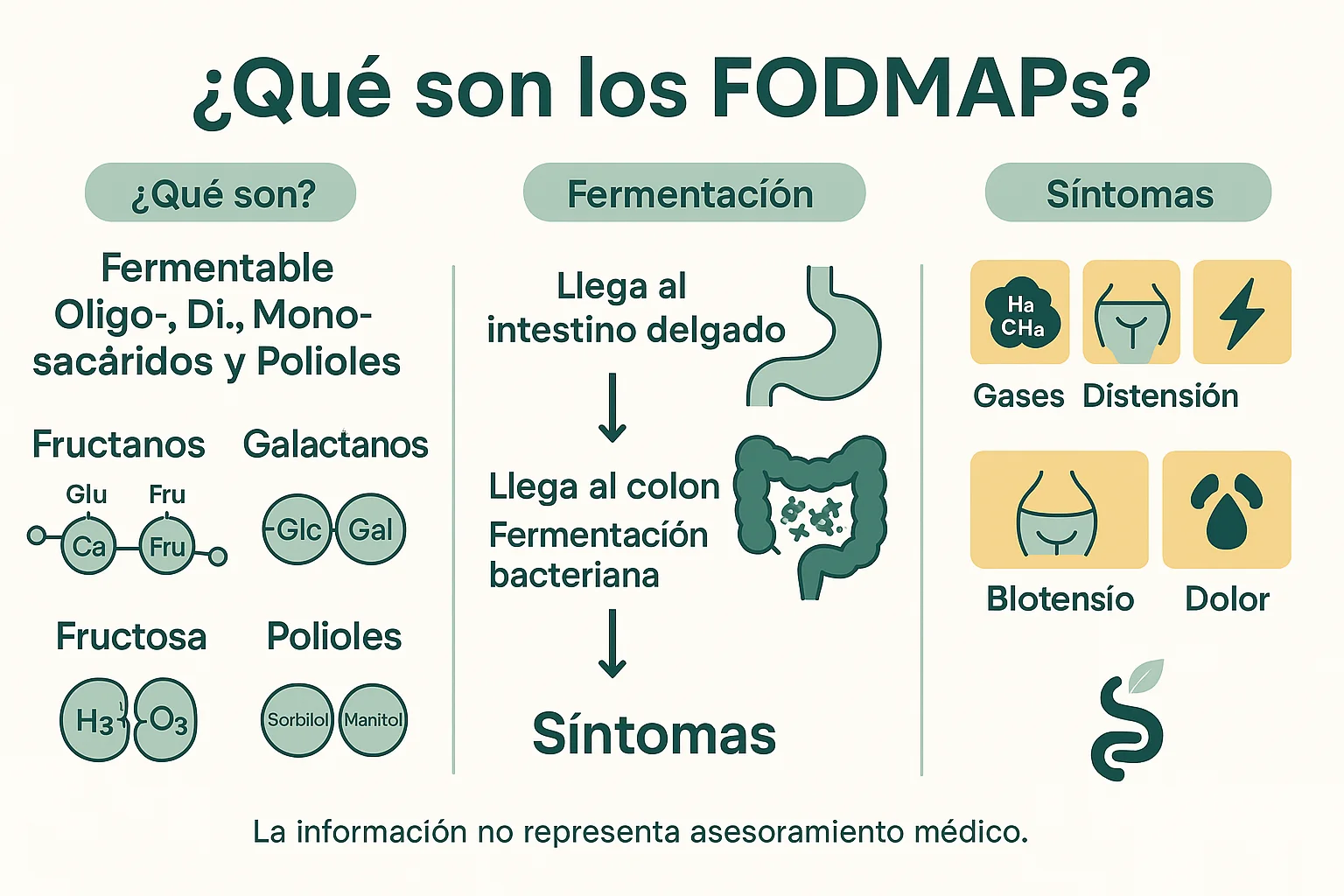
What are FODMAPs?
FODMAP is an acronym created by researchers at Monash University in Australia [3] that stands for:
- Fermentable (Fermentable)
- Oligosaccharides (Fructans and Galacto-oligosaccharides - GOS)
- Disaccharides (Lactose)
- Monosaccharides (Fructose in excess of glucose)
- Polyols (Sorbitol, Mannitol, Xylitol, Maltitol)
Why do they cause symptoms?
These short-chain carbohydrates have specific characteristics that make them problematic for people with SIBO or IBS:
- Poor absorption: They are poorly absorbed in the small intestine
- Osmotic: They draw water into the intestine, causing distension
- Fermentable: They are rapidly fermented by intestinal bacteria, producing gases (hydrogen, methane, carbon dioxide)
- Short chain: Their molecular structure allows rapid fermentation
Common symptoms caused by FODMAPs
- Abdominal bloating (distension)
- Excessive gas (flatulence)
- Abdominal pain and cramps
- Diarrhea or constipation
- Nausea
- Fatigue
- Early sense of fullness
Scientific Foundations of the Low-FODMAP Diet
Research and evidence
The Low-FODMAP diet was developed by researchers at Monash University in Melbourne, Australia, led by Dr. Peter Gibson and Dr. Sue Shepherd [3]. Since its introduction in 2005, it has been the subject of numerous scientific studies.
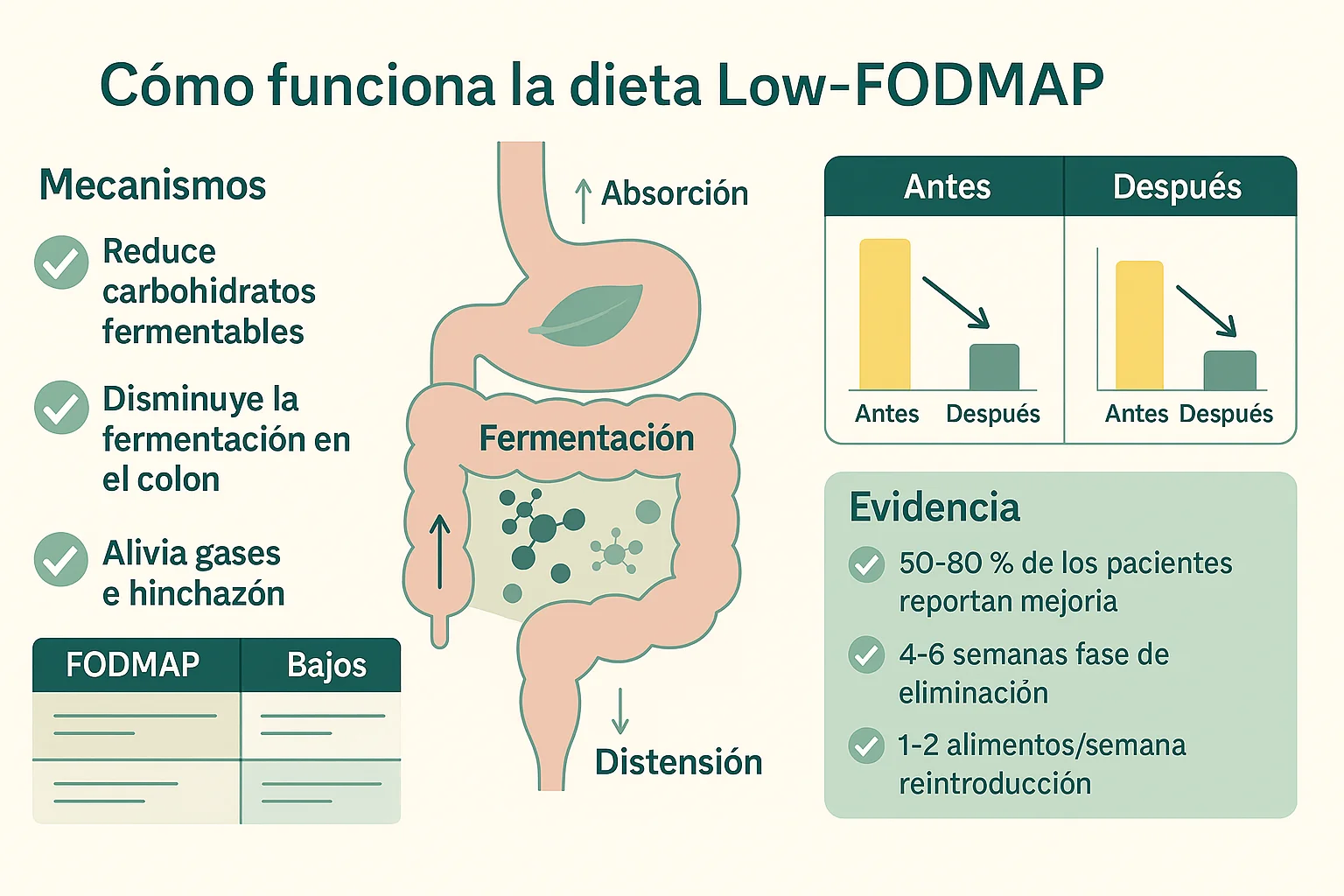
Current scientific evidence:
- 50-86% efficacy in reducing symptoms in patients with IBS [2]
- Positive response in 60-75% of patients with SIBO [1]
- Significant improvement in quality of life related to digestive health [2]
- Reduction of symptoms within 2-4 weeks in most cases [3]
Mechanisms of action
- Reduced fermentation: Less substrate for intestinal bacteria
- Lower osmolarity: Less water drawn into the intestine
- Reduced gas: Less production of hydrogen and methane
- Improved motility: Less distension improves intestinal movement
Phase 1: Elimination (2-6 weeks)
Main objective
Identify and temporarily eliminate all high-FODMAP foods in order to:
- Significantly reduce digestive symptoms
- Establish a baseline of well-being
- Prepare the gut for the reintroduction phase
- Identify whether FODMAPs are really a trigger
Recommended duration
- Minimum: 2 weeks (the time needed to see improvements)
- Maximum: 6 weeks (to avoid nutritional deficiencies) [3][4]
- Ideal: 3-4 weeks (the optimal balance between efficacy and safety)
⚠️ Warning: Do not stay in the elimination phase for more than 6 weeks without medical supervision. This phase is restrictive and can cause nutritional deficiencies if it is prolonged unnecessarily [3].
Editorial note: In practice, many people get “stuck” in the elimination phase out of fear of reintroducing foods. It’s understandable, but prolonging this phase beyond what is necessary can be counterproductive for the gut microbiota. If you’ve gone more than 4 weeks without progressing, talk to your dietitian about how to begin reintroduction gradually and adjusted to your case.
Foods to eliminate completely
High-FODMAP fruits
Fructans and Fructose:
- Apples (all varieties)
- Pears (all varieties)
- Mangoes
- Watermelons
- Cherries
- Figs
- Dates
Polyols:
- Peaches
- Plums
- Apricots
- Nectarines
- Lychees
Others:
- Canned fruit in juice
- Dried fruit (raisins, dates, dried figs)
- Concentrated fruit juices
High-FODMAP vegetables
Fructans:
- Onions (all varieties: white, yellow, red, sweet)
- Garlic (whole cloves)
- Leeks (the white part)
- Scallions
- Shallots
Fructans and GOS:
- Asparagus
- Artichokes (globe and Jerusalem)
- Brussels sprouts
- Cauliflower
- Peas (green peas)
Polyols:
- Mushrooms
- Cauliflower
- Celery (in large amounts)
- Beets
Others:
- Chives (in large amounts)
- Garlic powder and onion powder
High-FODMAP cereals and grains
Fructans:
- Wheat (bread, pasta, flour, couscous, bulgur)
- Rye (rye bread)
- Barley (except barley malt in small amounts)
- Spelt
- Kamut
Gluten products:
- White and whole-wheat bread
- Wheat pasta
- Cookies and bakery products
- Wheat-based breakfast cereals
- Flour tortillas
High-FODMAP legumes
GOS (Galacto-oligosaccharides):
- Beans (black, pinto, red, white)
- Lentils (except canned and rinsed in small portions)
- Chickpeas (except canned and rinsed in small portions)
- Soy and its derivatives (silken tofu, soy milk)
- Split peas
- Lupins
- Soybeans (except edamame in small portions)
High-FODMAP dairy
Lactose:
- Cow’s milk (whole, skim, semi-skim)
- Sheep’s and goat’s milk
- Soft cheeses with lactose (ricotta, cottage, fresh cheese)
- Yogurt with lactose (regular, Greek with lactose)
- Sour cream
- Cream (heavy cream)
- Ice creams with lactose
- Condensed and evaporated milk
High-FODMAP sweeteners
Fructose:
- Honey (all varieties)
- Agave syrup
- High-fructose corn syrup
- Agave nectar
- Maple syrup (in large amounts)
Polyols:
- Sorbitol (E420)
- Mannitol (E421)
- Xylitol (E967)
- Maltitol (E965)
- Isomalt (E953)
- Erythritol (in large amounts)
Others:
- Pure fructose
- Concentrated fruit syrups
High-FODMAP nuts and seeds
GOS and Fructans:
- Cashews
- Pistachios
- Hazelnuts
- Almonds (in large amounts - more than 10 units)

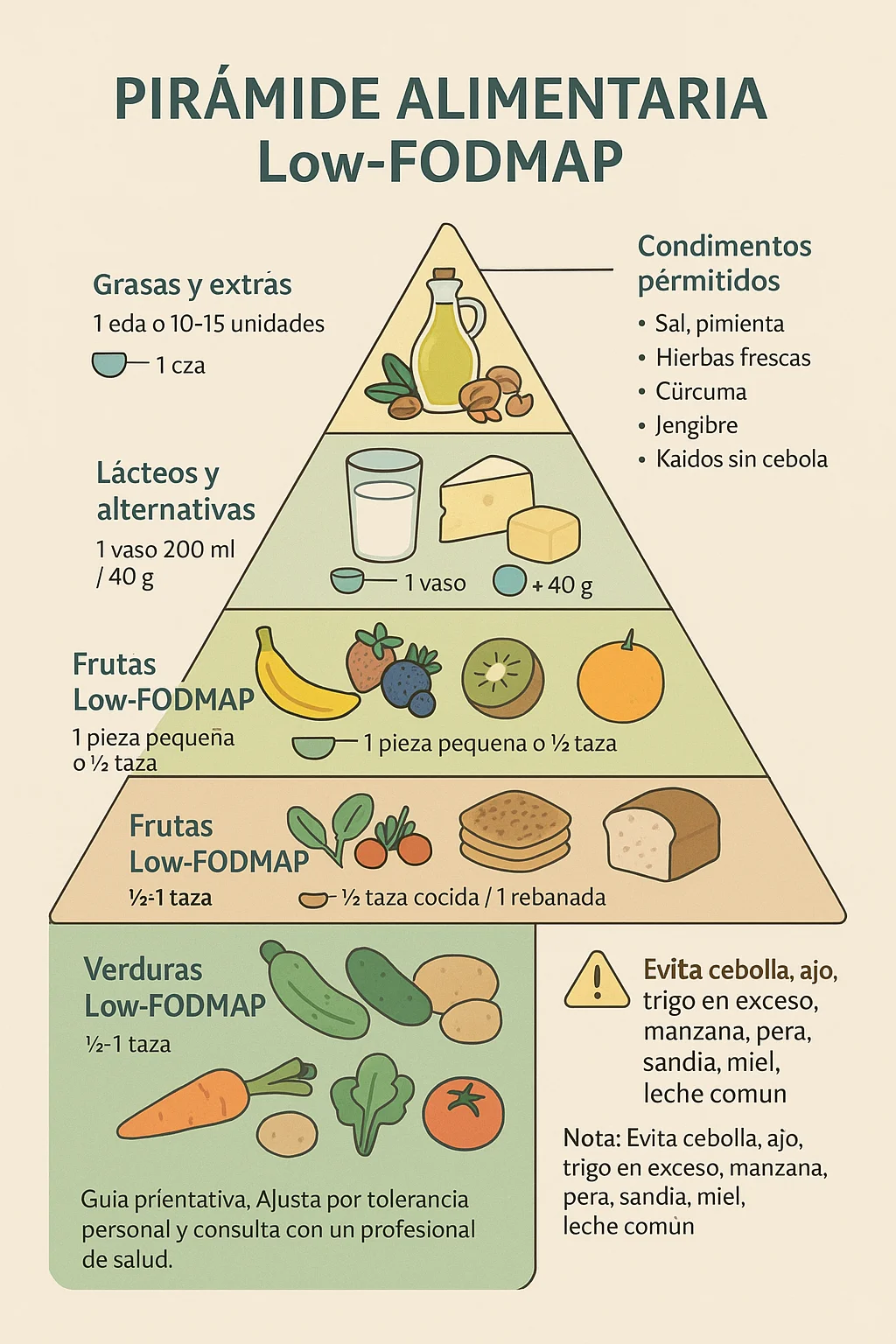
Visual summary of foods that are usually avoided and foods that are usually allowed during the low-FODMAP phase.
Allowed foods (Low-FODMAP)
Low-FODMAP fruits
Low in FODMAPs in approximate portions:
- Bananas (ripe, up to 100g)
- Blueberries (up to 40g)
- Strawberries (up to 5 medium units)
- Oranges (up to 150g)
- Mandarins (up to 150g)
- Kiwis (up to 150g)
- Lemons and limes
- Grapes (up to 75g, seedless)
- Pineapple (up to 140g)
- Papaya (up to 140g)
- Passion fruit (up to 50g)
- Star fruit (up to 100g)
Low-FODMAP vegetables
Low in FODMAPs in approximate portions:
- Carrots
- Cucumbers
- Zucchini
- Lettuce (all varieties)
- Spinach
- Tomatoes (cherry tomatoes are usually better tolerated in measured portions)
- Potatoes
- Squash (pumpkin)
- Bell peppers (red, green, yellow)
- Eggplant
- Green beans
- Ginger
- Radishes
- Bamboo shoots
- Bok choy
- Cabbage (white and red)
- Kale
- Arugula
Gluten-free cereals and grains
Low in FODMAPs or gluten-free in approximate portions:
- White and brown rice
- Quinoa
- Gluten-free oats (up to 52g rolled)
- Corn (up to 38g - half a small cob)
- Millet
- Sorghum
- Buckwheat
- Amaranth
- Teff
- Corn tortillas (gluten-free)
- Rice cakes
- Puffed rice cereals
Low-FODMAP proteins
All proteins are naturally low in FODMAPs:
- Lean meat (chicken, turkey, beef, pork, lamb)
- Fish (white and oily)
- Shellfish (shrimp, lobster, crab, mussels, clams)
- Eggs
- Firm tofu (pressed and drained)
- Tempeh (up to 75g)
Lactose-free dairy
Lactose-free or naturally low-lactose options:
- Lactose-free milk
- Almond milk (without carrageenan)
- Rice milk
- Coconut milk (canned, only the solid part - up to 125g)
- Hard cheeses (cheddar, parmesan, Swiss, mozzarella, feta, brie, camembert)
- Lactose-free yogurt
- Lactose-free kefir
- Lactose-free cream cheese
- Lactose-free sour cream
Low-FODMAP nuts and seeds
In controlled portions:
- Walnuts (up to 30g - 10 halves)
- Peanuts (up to 30g)
- Brazil nuts (up to 30g)
- Macadamia nuts (up to 40g)
- Pecans (up to 20g)
- Pine nuts (up to 20g)
- Almonds (up to 10 units)
- Peanut butter (no added sugars)
- Almond butter (up to 20g)
- Chia seeds (up to 15g - 2 tablespoons)
- Flax seeds (ground, up to 15g)
- Sesame seeds (up to 15g)
- Pumpkin seeds (up to 20g)
- Sunflower seeds (up to 20g)
Low-FODMAP sweeteners
Low-FODMAP options in approximate portions:
- White sugar (sucrose)
- Brown sugar
- Maple syrup - up to 50g
- Stevia
- Coconut sugar (in small amounts - up to 5g)
What to expect during the elimination phase
First week
Days 1-3:
- Gradual reduction of symptoms
- Possible temporary constipation (normal due to the change in diet)
- Adjustment of the digestive system to the new way of eating
- There may be initial fatigue while the body adapts
Days 4-7:
- More noticeable improvement of symptoms
- Reduction of bloating and gas
- Establishment of new eating patterns
- Possible need to adjust portions
Second week onward
Weeks 2-3:
- Significant and sustained improvement of symptoms
- Greater energy and general well-being
- Establishment of a symptom baseline
- Greater confidence in the diet
Weeks 4-6:
- Minimal or absent symptoms (if FODMAPs were the problem)
- Digestive stability
- Mental preparation for reintroduction
When to move to phase 2 (Reintroduction)
You can move on to reintroduction when you meet ALL of these criteria:
- ✅ Symptom improvement: Symptoms have improved by at least 50% compared to the start
- ✅ Minimum time: You have completed at least 2 weeks in the elimination phase
- ✅ Stability: You feel stable and comfortable with the Low-FODMAP diet
- ✅ Medical supervision: You have consulted with your doctor or dietitian and they have given the green light
- ✅ Controlled symptoms: Symptoms are under control and manageable
⚠️ Do not move on to phase 2 if:
- Symptoms have not improved significantly
- You are experiencing new or severe symptoms
- Your doctor has not approved it
- You have not completed at least 2 weeks
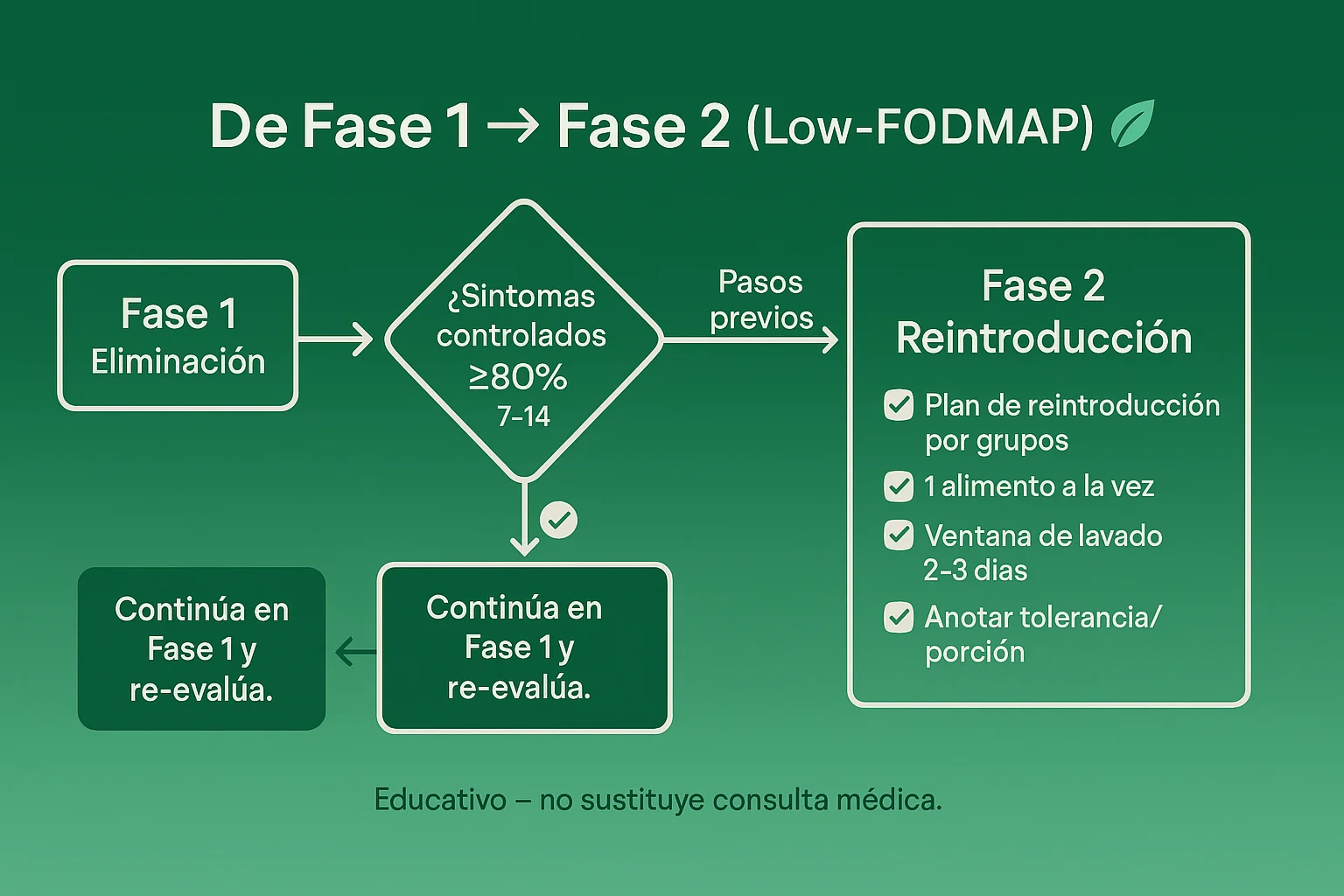
Phase 2: Systematic Reintroduction (6-8 weeks)
Main objective
Identify which specific FODMAP groups cause symptoms and in what amounts you can tolerate them [3][4]. This phase is CRITICAL and must be done in a systematic, controlled way.
Why reintroduction is important
- Avoid unnecessary restrictions: Many people tolerate some FODMAP groups
- Nutritional variety: It allows a more balanced and complete diet
- Sustainability: A less restrictive diet is easier to maintain over the long term
- Precise identification: It lets you know exactly which foods to avoid
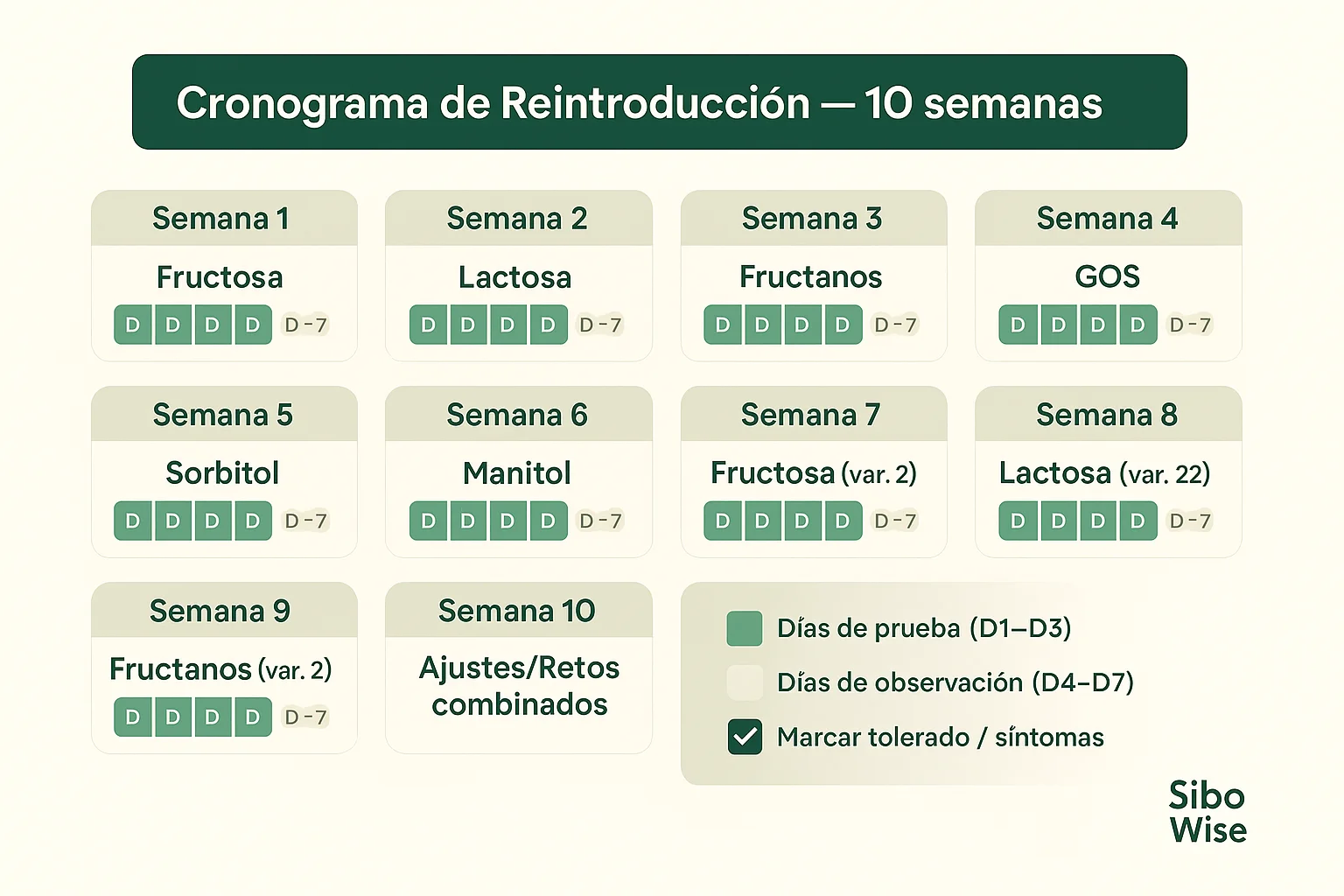
Methodology: Testing by groups
Reintroduction must be done one group at a time, testing specific foods from each FODMAP category.
Weeks 1-2: Fructans (Group 1)
What are fructans? Carbohydrates made of chains of fructose found in wheat, onion, garlic, and other vegetables.
Test foods:
- Day 1: Wheat bread (1 small slice - 25g)
- Days 2-3: Observe symptoms without testing any other new foods
- If there are no symptoms: Try 2 slices on day 4
- If there are symptoms: Note the amount and type of symptoms, avoid fructans for now
Other fructan-containing foods to test later:
- Wheat pasta (small portion)
- Cooked onion (small amount)
- Garlic in oil (flavor without FODMAPs, but test real garlic afterward)
Weeks 3-4: Lactose (Group 2)
What is lactose? A disaccharide found in dairy products that requires the enzyme lactase to be digested.
Test foods:
- Day 1: Lactose-free milk mixed with regular milk (50ml of regular milk)
- Days 2-3: Observe symptoms
- If there are no symptoms: Gradually increase to 100ml, then 150ml
- If there are symptoms: Note the amount tolerated
Other lactose-containing foods to test later:
- Yogurt with lactose (small portion)
- Soft cheese with lactose (ricotta, cottage)
- Ice cream with lactose (small portion)
Weeks 5-6: Fructose (Group 3)
What is fructose? A monosaccharide (simple sugar) found in fruit and some sweeteners.
Test foods:
- Day 1: Honey (1 teaspoon - 5g)
- Days 2-3: Observe symptoms
- Day 4: Small apple (if there were no symptoms with honey)
- If there are symptoms: Note which food and amount caused symptoms
Other fructose-containing foods to test later:
- Small pear
- Mango (small portion)
- Agave syrup (small amount)
Weeks 7-8: Polyols (Group 4)
What are polyols? Sugar alcohols found in some fruits and artificial sweeteners.
Subgroup A: Sorbitol
- Day 1: Avocado (1/4 of a medium avocado - 30g)
- Days 2-3: Observe symptoms
- If there are no symptoms: Try a small peach
Subgroup B: Mannitol
- Day 1: Mushrooms (small portion - 50g)
- Days 2-3: Observe symptoms
- If there are no symptoms: Try a small amount of cauliflower
Subgroup C: Artificial polyols
- Xylitol, sorbitol, mannitol in sugar-free products
- Test in very small amounts
Weeks 9-10: GOS - Galacto-oligosaccharides (Group 5)
What are GOS? Carbohydrates found mainly in legumes.
Test foods:
- Day 1: Canned and rinsed chickpeas (42g - 1/4 cup)
- Days 2-3: Observe symptoms
- If there are no symptoms: Try canned and rinsed lentils (46g)
- If there are symptoms: GOS may be problematic for you
Detailed testing protocol
Step 1: Preparation
- Choose a quiet day: Don’t test new foods on stressful days or days with important events
- Prepare the food: Have the test food ready in the exact amount
- Prepare your journal: Have your symptom journal ready to record everything
- Eat normally: Keep the rest of your Low-FODMAP diet unchanged
Step 2: Testing the food
- Eat a small portion: Start with the recommended “low FODMAP” portion
- Eat only that new food: Don’t combine it with other new foods
- Record immediately: Note the exact time and the amount consumed
Step 3: Observation (48-72 hours)
Day 1 (test day):
- Observe symptoms in the first 2-4 hours
- Record any change in digestive symptoms
- Continue with your normal Low-FODMAP diet
Days 2-3 (observation days):
- DO NOT test other new foods
- Keep your normal Low-FODMAP diet
- Observe ongoing or delayed symptoms
- Record everything in your journal
Step 4: Evaluation
If there are NO symptoms:
- ✅ The food is tolerated in that amount
- Test a larger portion after 3 days
- Keep increasing gradually until you find your threshold
If there ARE symptoms:
- ❌ The food causes symptoms in that amount
- Note the type and severity of symptoms
- Wait until the symptoms disappear completely
- Test the next FODMAP group after one week
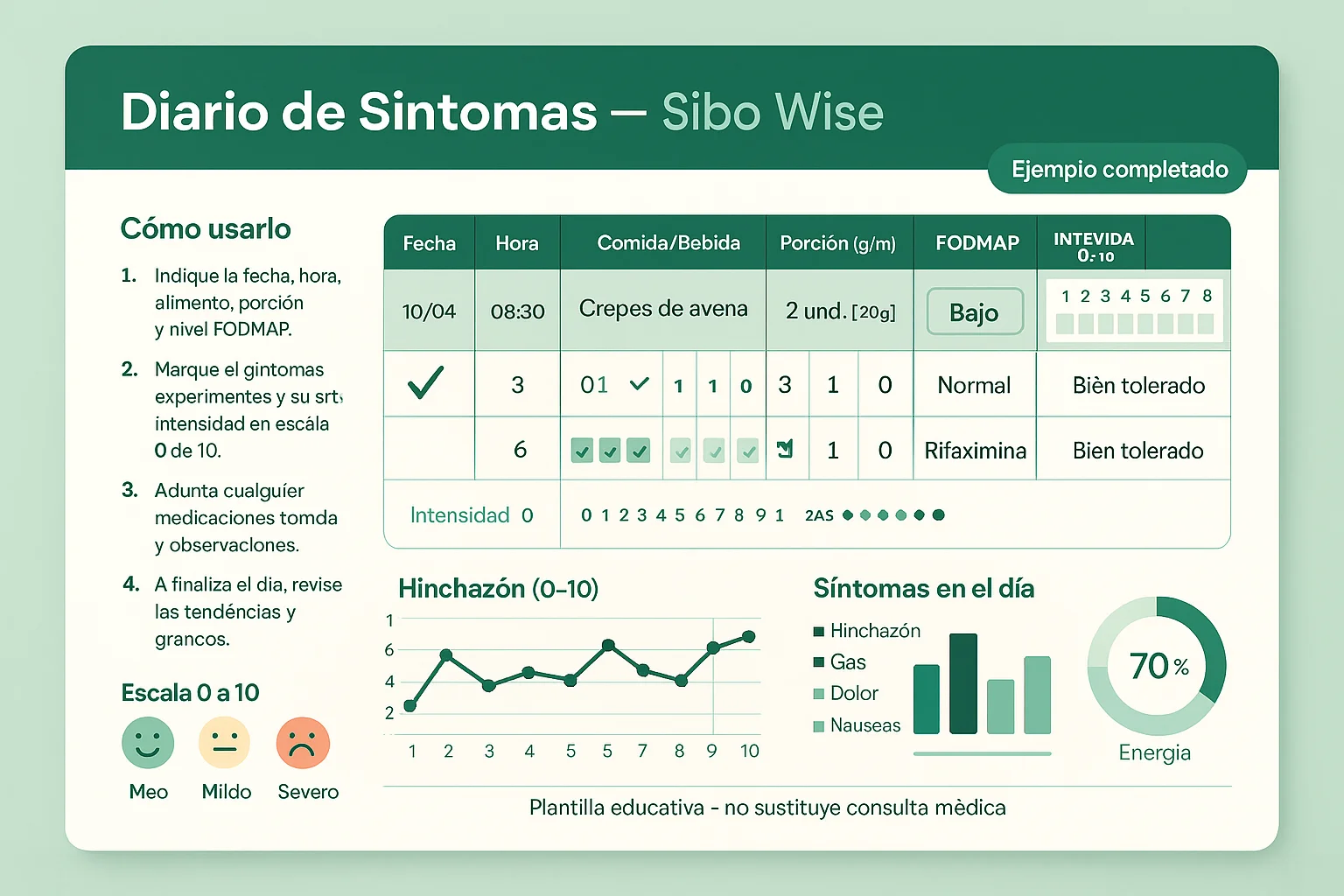
Symptom tracking: A detailed journal
Keep a thorough journal with the following information:
Food information
- Exact date and time of the test
- Food tested and FODMAP group
- Exact amount consumed (in grams or household measures)
- Method of preparation (raw, cooked, etc.)
Symptoms experienced
- Type of symptom (bloating, gas, pain, diarrhea, constipation, nausea)
- Severity on a 0-10 scale (0 = no symptoms, 10 = severe symptoms)
- Time until onset of symptoms (minutes or hours)
- Duration of symptoms
- Maximum intensity of the symptom
Contextual factors
- Stress level of the day
- Sleep quality the night before
- Exercise performed
- Other foods consumed that day
- Medications or supplements taken
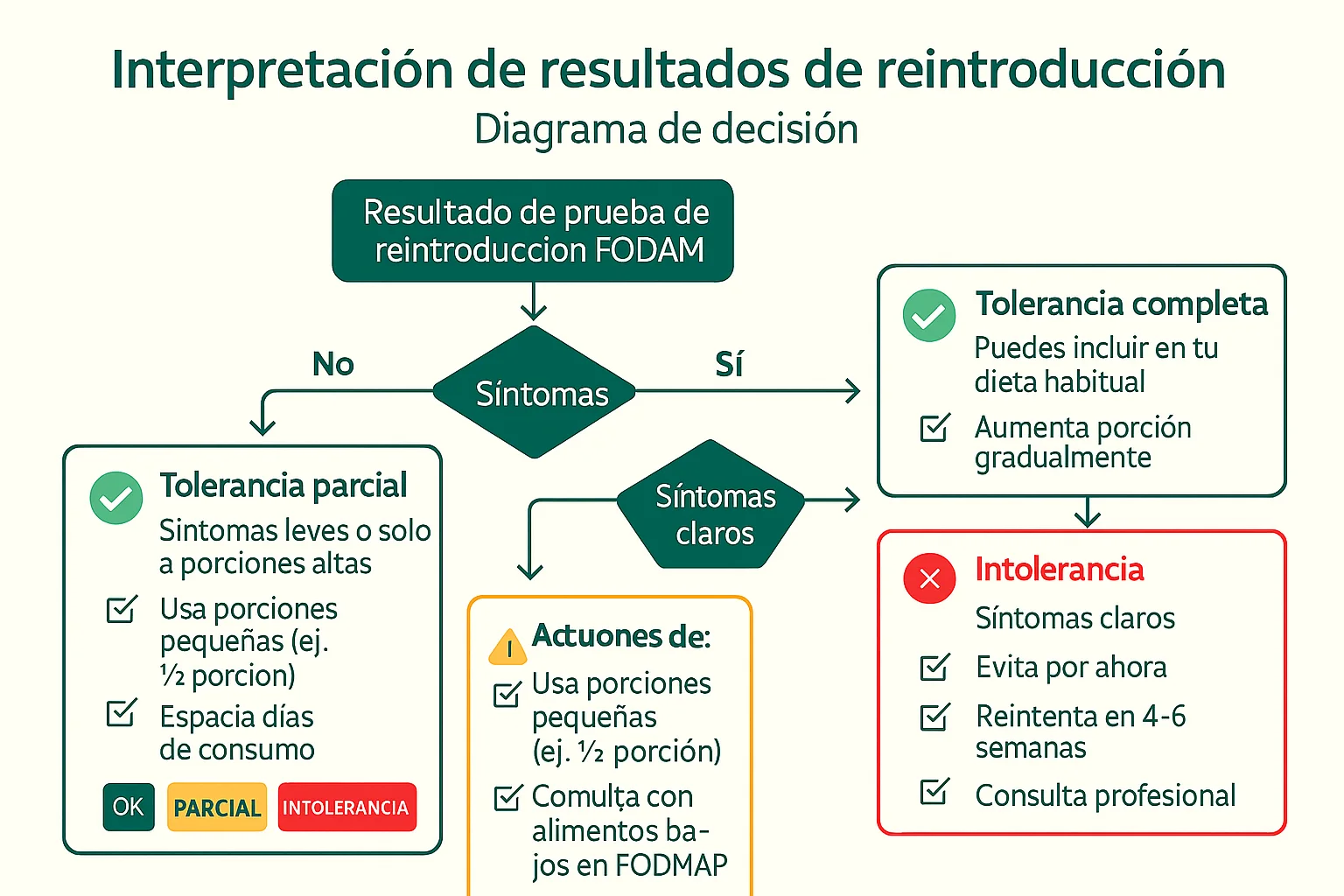
Interpreting results
Full tolerance ✅
Characteristics:
- No symptoms with normal portions of the food
- You can eat the food regularly without restrictions
- You don’t need to limit the amount or frequency
Action:
- Include this FODMAP group in your regular diet
- You don’t need to avoid it in phase 3
Partial tolerance ⚠️
Characteristics:
- Symptoms only with large portions
- You can tolerate small amounts without problems
- The threshold is clear and defined
Action:
- Limit the amount to your identified personal threshold
- Control the frequency of consumption
- Combine strategically with other low-FODMAP foods
- Cross-check portions with up-to-date sources and with your health professional’s judgment
Intolerance ❌
Characteristics:
- Symptoms even with very small portions
- A consistent reaction every time you consume the food
- Severe or moderate symptoms
Action:
- Avoid this FODMAP group in phase 3
- Or consume it very occasionally and with planning
- Look for Low-FODMAP alternatives
- Consider working with a dietitian to find nutritional substitutes
Common mistakes during reintroduction
❌ Mistake 1: Testing multiple foods at once
Problem: If you test several new foods at the same time, you won’t be able to identify which one causes symptoms.
Solution: Test ONE food at a time, wait 3 days before testing another.
❌ Mistake 2: Portions that are too large
Problem: Starting with large portions can cause severe symptoms and make it hard to identify your real threshold.
Solution: Always start with small portions (the “low FODMAP” portion) and increase gradually.
❌ Mistake 3: Not waiting long enough
Problem: Symptoms can appear up to 48 hours after consuming the food.
Solution: Wait at least 3 days between tests of new foods.
❌ Mistake 4: Not recording properly
Problem: Without a detailed record, it’s hard to identify patterns and thresholds.
Solution: Keep a thorough journal with all the relevant information.
❌ Mistake 5: Reintroducing too quickly
Problem: Wanting to speed up the process can lead to confusing results and uncontrolled symptoms.
Solution: Be patient and systematic. Reintroduction takes time but it is essential.
Phase 3: Long-Term Personalization
Main objective
Create a personalized diet that maximizes nutritional variety while minimizing symptoms [3]. This phase is for life and must be flexible and sustainable.
Fundamental principles
1. Nutritional variety
Importance:
- Avoids nutritional deficiencies
- Keeps an interest in food
- Provides all the necessary nutrients
- Supports general health
Strategies:
- Include foods from all the allowed groups
- Prioritize fresh, natural foods
- Avoid unnecessary restrictions based on fears
- Rotate foods regularly
2. Individual portions
Key concept: Each person has different thresholds for each FODMAP group.
Practical application:
- Respect your personal thresholds identified in phase 2
- Use personal records and up-to-date sources to plan prudently
- Learn to combine foods strategically
- Don’t assume that “a little more” will be fine without testing it
3. Food rotation
Benefits:
- Avoids developing new sensitivities
- Lets the gut adapt gradually
- Keeps variety in the diet
- Reduces the risk of nutritional deficiencies
Strategy:
- Don’t eat the same food every day
- Vary your nutrient sources (e.g., different vegetables each day)
- Allow “rest” days for problematic foods
- Plan varied meals throughout the week
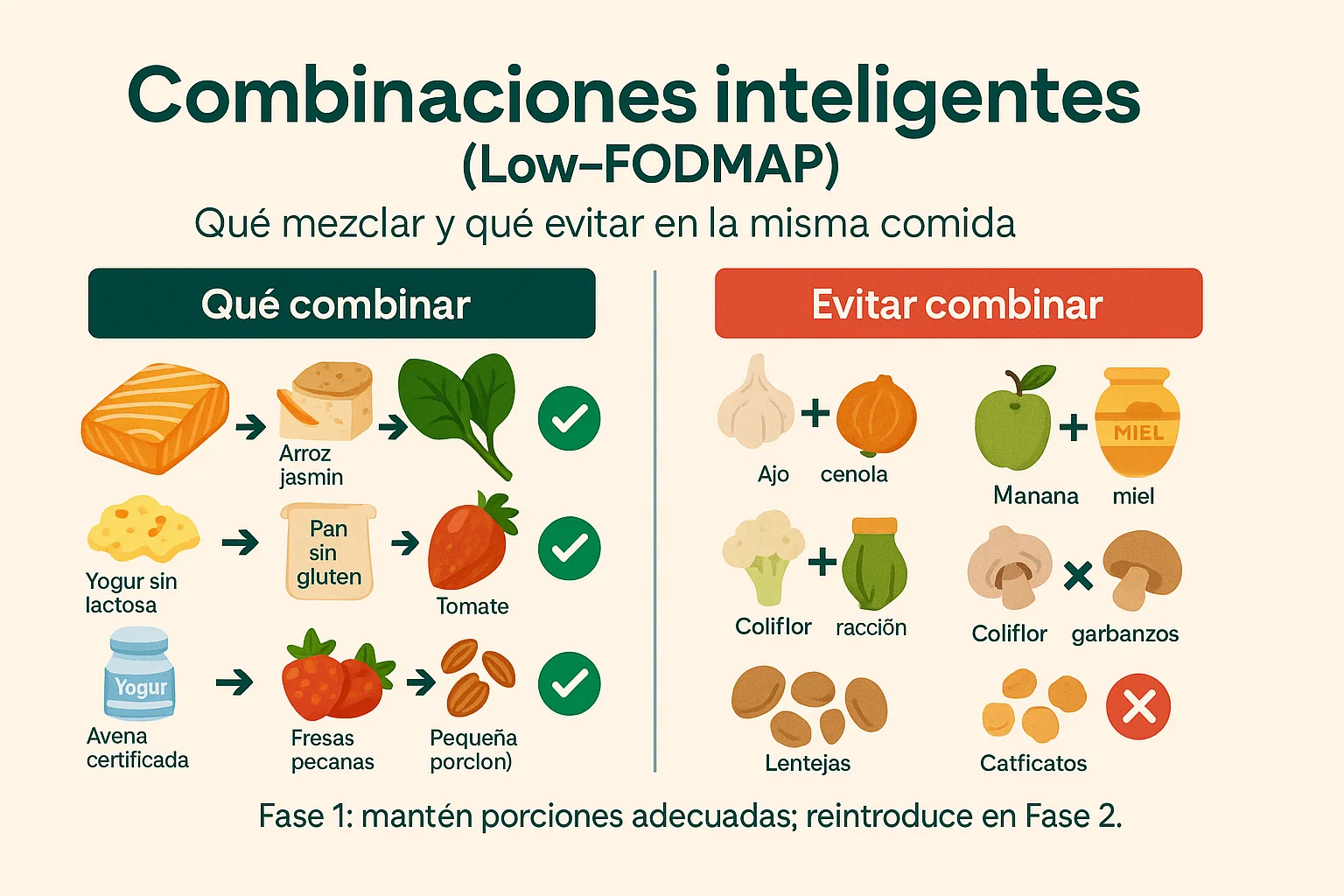
4. Combination strategies
Principle: The accumulation of FODMAPs can cause symptoms even if each individual food is within a low-FODMAP portion.
Basic rules:
- Combine low-FODMAP foods freely
- Spread problematic foods throughout the day
- Avoid accumulating multiple sources of the same FODMAP in one meal
- Review combinations with up-to-date sources and avoid accumulating several fermentable groups in the same meal
Example of smart combining:
- ✅ Good: Chicken + rice + carrots + spinach (all low in FODMAPs)
- ⚠️ Caution: Avocado (sorbitol) + peach (sorbitol) in the same meal
- ✅ Better: Avocado at breakfast, peach as a separate snack
Foods you can reintroduce gradually
With identified partial tolerance
Sourdough bread:
- Prolonged fermentation reduces FODMAPs
- Test small portions first
- Observe your individual tolerance
Oats:
- In controlled portions (up to 52g rolled)
- Make sure it is certified gluten-free
- Test gradually
Canned and rinsed legumes:
- Chickpeas: up to 42g (1/4 cup)
- Lentils: up to 46g (1/4 cup)
- Black beans: up to 40g (1/4 cup)
- Important: Rinse well to reduce GOS
Some high-FODMAP fruits:
- In very small portions if you tolerated them partially
- Example: 1/4 of a small apple if you tolerated honey
- Always respect your personal threshold
With proper preparation
Garlic and onion in oil:
- Infuse oil with garlic/onion, then remove the solids
- You get the flavor without the FODMAPs
- Use it for cooking and seasoning
Asparagus:
- Only the tips (the most tender part)
- In small portions (up to 3-4 tips)
- Avoid the stalks, which are higher in FODMAPs
Broccoli:
- Only the florets (the top part)
- Avoid the stalks, which are higher in fructans
- Up to 75g of cooked florets
Tomatoes:
- Cherry tomatoes are usually easier to measure than large ones
- Up to 150g of cherry tomatoes
- Large tomatoes can be problematic in large amounts
Long-term maintenance
Successful strategies
1. Weekly planning
- Organize your meals by week with a simple, flexible list
- Prepare meals in advance when possible
- Keep Low-FODMAP snacks available for emergencies
- Plan meals away from home in advance
2. Ongoing education
- Stay up to date on new foods and their FODMAP content
- Read labels carefully (ingredients change)
- Consult reliable resources such as the Monash University app
- Join support communities (with caution about medical advice)
3. Professional support
- Visit your specialized dietitian regularly
- Monitor your progress with your gastroenterologist
- Adjust according to changes in symptoms or health conditions
- Don’t hesitate to seek help if symptoms get worse
4. Smart flexibility
- Allow yourself special occasions with prior planning
- Learn to handle “mistakes” without excessive guilt
- Recognize that the diet is a tool, not a prison
- Balance restrictions with quality of life
Common Mistakes and How to Avoid Them
❌ Mistake 1: Elimination that lasts too long
Problem: Staying in phase 1 for more than 6 weeks can cause:
- Nutritional deficiencies (fiber, calcium, iron, vitamin D)
- Unnecessary restrictions
- Difficulty identifying real tolerances
- Negative impact on the gut microbiota
Solution:
- Move on to reintroduction after 2-4 weeks if symptoms improve
- Work with a dietitian to ensure nutritional adequacy
- Do not stay in elimination for more than 6 weeks without medical supervision
❌ Mistake 2: Reintroducing too quickly
Problem: Testing multiple new foods in a short time:
- Makes it hard to identify what causes symptoms
- Can cause severe symptoms and confusion
- Makes the results unreliable
- Can lead to unnecessary restrictions out of fear
Solution:
- Test one food every 3 days
- Keep a detailed record
- Be patient and systematic
- Don’t rush the process
❌ Mistake 3: Unnecessary restrictions
Problem: Eliminating foods you actually tolerate:
- Unnecessarily reduces nutritional variety
- Makes the diet harder to maintain
- Can cause nutritional deficiencies
- Reduces quality of life without benefit
Solution:
- Systematically reintroduce all the groups
- Test your personal limits in a controlled way
- Trust the results of your tests
- Don’t eliminate foods “just in case”
❌ Mistake 4: Ignoring portions
Problem: Many foods can fit within small portions but become problematic in large portions:
- You may be avoiding foods you could tolerate
- Or consuming too much of foods considered low in FODMAPs
- The accumulation can cause symptoms
Solution:
- Review portions with up-to-date sources and with the recipe-book methodology
- Respect the recommended portions
- Learn to measure portions visually
- Consider using a kitchen scale at first
❌ Mistake 5: Not considering combinations
Problem: Eating multiple low-FODMAP foods can add up and cause symptoms:
- Several low-FODMAP foods can add up the fermentable load
- The combination can exceed your personal threshold
- It can cause confusion about which food caused symptoms
Solution:
- Plan balanced meals
- Spread problematic foods throughout the day
- Review combinations with a gradual approach and avoid making too many changes at once
- Learn which FODMAP groups accumulate
❌ Mistake 6: Self-diagnosis without supervision
Problem: Trying to do the diet without medical supervision:
- Can lead to incorrect diagnoses
- Can cause nutritional deficiencies
- Can delay proper treatment of underlying conditions
- Can cause unnecessary anxiety and stress
Solution:
- Always work with a gastroenterologist
- Consult a dietitian specialized in FODMAPs
- Don’t use the diet as the only treatment without a medical diagnosis
- Keep regular communication with your health team
Supplementation during the Low-FODMAP Diet
Important considerations
The elimination phase can be restrictive and may require supplementation to prevent nutritional deficiencies. Always consult your doctor or dietitian before taking any supplement.
Nutrients that may need attention
Vitamin D
Why it may be necessary:
- Reduced sun exposure
- Lower intake of fortified foods
- Important for bone health and immunity
Low-FODMAP sources:
- Fatty fish (salmon, tuna)
- Eggs
- Fortified lactose-free milk
- Supplementation if necessary (medical consultation)
Calcium
Why it may be necessary:
- Restriction of dairy with lactose
- Important for bone health
Low-FODMAP sources:
- Lactose-free dairy (milk, yogurt, cheese)
- Fish with bones (canned sardines)
- Firm tofu (prepared with calcium)
- Leafy green vegetables (spinach, kale)
- Supplementation if necessary (medical consultation)
Iron
Why it may be necessary:
- Restriction of some iron sources
- Important for preventing anemia
Low-FODMAP sources:
- Lean meats (chicken, beef, pork)
- Fish
- Spinach
- Eggs
- Combine with vitamin C to improve absorption (oranges, bell peppers)
Fiber
Why it may be necessary:
- The diet can be low in fiber if it isn’t planned well
- Important for digestive health and regularity
Low-FODMAP sources:
- Gluten-free oats
- Quinoa
- Brown rice
- Allowed vegetables (spinach, carrots, zucchini)
- Chia and flax seeds (in controlled portions)
Probiotics
Probiotics are not a universal recommendation. Some people tolerate them well and others notice more symptoms, depending on the product, the strain, the excipients, and the clinical moment.
Before adding them, check with your health team whether they make sense in your case and verify that they do not include high-FODMAP ingredients.

Integration with Professional Care
Teamwork: A comprehensive approach
The Low-FODMAP diet is a dietary management tool. It does not confirm diagnoses or replace the evaluation of underlying causes.
Editorial note: A common misconception is to think that a diet on its own resolves all digestive symptoms. In reality, its main function is to explore tolerance and reduce fermentable load while the clinical context is reviewed.
Points your team may review
Associated conditions:
- Hypochlorhydria (low stomach acid)
- Ileocecal valve dysfunction
- Chronic constipation
- Other conditions that predispose to SIBO
Habits and context
Stress management:
- Stress can worsen digestive symptoms
- Relaxation techniques (meditation, deep breathing)
- Psychological therapy if necessary
- Regular exercise (moderate, not excessive)
Regular exercise:
- It can support general well-being and help maintain routines.
- It is best to adjust it to your energy, symptoms, and physical condition.
- Intense exercise can worsen symptoms in some people.
Adequate sleep:
- 7-9 hours of quality sleep
- Regular sleep helps regulate the digestive system
- Lack of sleep can worsen symptoms
Adequate hydration:
- Drink enough water (but not in excess during meals)
- Avoid beverages high in FODMAPs
- Water helps with intestinal motility
Regular follow-up
Periodic medical visits:
- Gastroenterologist: every 3-6 months or as needed
- Dietitian: regularly during phases 1 and 2, then as needed
- Monitoring of symptoms and adjustments to the plan
Adjustments as things evolve:
- The diet may need adjustments based on changes in symptoms
- The medical or nutritional plan may require modifications
- Health conditions change over time
Symptom monitoring:
- Keep a regular symptom journal
- Identify patterns and triggers
- Communicate changes to your medical team

Sibo Wise Resources
Recipe-book methodology
Check our Low-FODMAP methodology to:
- Understand the criteria: how we classify recipes and why the portions are approximate
- Avoid false certainties: a low-FODMAP recipe does not guarantee individual tolerance
- Use portions prudently: adjust amounts according to tolerance, phase, and clinical context
- Look for alternatives: compare recipes with simpler ingredients when a preparation doesn’t work for you
How to use this methodology:
- Review the criteria before using a recipe as a reference.
- Start with prudent portions if you are in a restrictive phase.
- Record your real tolerance instead of assuming a label applies the same way to everyone.
- Take persistent questions to your health professional.
Weekly organization
You can set up a simple weekly plan to:
- Organize the week’s meals: Plan breakfasts, lunches, dinners, and snacks
- Ensure nutritional variety: Make sure you’re eating from all the groups
- Make preparation easier: Have a clear plan for shopping and preparation
- Maintain the diet: A clear plan makes it easier to follow the diet
Benefits of getting organized:
- Reduces the stress of “what do I eat today?”
- Makes food shopping easier
- Allows advance preparation
- Helps maintain nutritional variety
Low-FODMAP recipe book
Explore our recipe book with:
- Recipes with Low-FODMAP criteria: The recipes use approximate portions and must be adjusted to individual tolerance
- Complete nutritional information: Calories, macronutrients, portions
- Clearly indicated FODMAP levels: You know exactly what you’re eating
- A variety of options: Breakfasts, lunches, dinners, snacks, desserts
How to use the recipe book:
- Search for recipes by category or ingredient
- Filter by FODMAP level if necessary
- Save your favorite recipes
- Use them within your weekly organization
Frequently Asked Questions (FAQ)
How long should I stay in each phase?
Phase 1 (Elimination): 2-6 weeks, ideally 3-4 weeks Phase 2 (Reintroduction): 6-8 weeks, can be extended up to 10-12 weeks if necessary Phase 3 (Personalization): For life, with adjustments as needed
Can I skip the reintroduction phase?
It is not recommended. The reintroduction phase is essential to:
- Identify your personal tolerances
- Avoid unnecessary restrictions
- Create a sustainable long-term diet
- Maximize nutritional variety
What if I don’t improve during the elimination phase?
If you don’t improve after 4-6 weeks in the elimination phase:
- FODMAPs may not be your main problem
- There may be other conditions that need treatment
- Consult your doctor to reassess
- Another dietary approach or medical treatment may be necessary
Can I do the Low-FODMAP diet if I am pregnant or breastfeeding?
Always consult your doctor first. The diet can be restrictive and:
- May require modifications during pregnancy
- May affect the baby’s nutrition during breastfeeding
- Requires close medical supervision
- May not be appropriate in all cases
Does the Low-FODMAP diet cure SIBO?
No. The Low-FODMAP diet is a dietary tool to explore tolerance and reduce fermentable load. It does not diagnose or cure SIBO, and it does not replace professional evaluation.
Can I eat out while following the diet?
Yes, with planning:
- Look up the menu before you go
- Call the restaurant in advance
- Ask for modifications (no onion, no garlic, etc.)
- Choose options that are simpler to review (grilled meats, simple salads)
- Keep Low-FODMAP snacks with you just in case
What do I do if I accidentally eat something high in FODMAPs?
Don’t panic:
- Note what you ate and how much
- Watch for symptoms
- Return to your normal Low-FODMAP diet
- Wait for the symptoms to disappear before testing something new
- Learn from the experience for the future
Is the Low-FODMAP diet forever?
Not necessarily. Phase 3 (personalization) is long-term, but:
- Many people can expand their diet gradually
- Some people may need to maintain restrictions
- The diet should adapt to changes in symptoms and health
- Work with your medical team to adjust as needed
Conclusion
The Low-FODMAP diet is a powerful, scientifically supported tool when applied correctly under medical supervision. The three phases - elimination, systematic reintroduction, and long-term personalization - work together to help you:
- ✅ Identify your specific FODMAP triggers
- ✅ Create a sustainable diet that supports your digestive well-being
- ✅ Maximize nutritional variety while minimizing symptoms
- ✅ Improve your quality of life and general well-being
Important final reminders
- Medical supervision is essential: Do not attempt this diet without professional supervision
- Be patient: The process takes time but it’s worth it
- Keep records: A detailed journal is your best tool
- Be flexible: The diet is a tool, not a prison
- Seek support: Work with professionals and consider support groups
- Trust the process: Systematic reintroduction is key to long-term success
Next steps
- Consult your gastroenterologist about whether the Low-FODMAP diet is appropriate for you
- Work with a dietitian specialized in FODMAPs
- Start phase 1 (elimination) when you have the medical green light
- Use the Sibo Wise recipe book and methodology as educational support, without replacing professional guidance
- Keep a symptom journal from day one
- Be patient and systematic during the reintroduction phase
Additional resources
- Monash University: Creators of the Low-FODMAP diet - monashfodmap.com
- Monash FODMAP App: The official FODMAP food database
- Sibo Wise Methodology: Low-FODMAP recipe-book criteria
- Sibo Wise Recipe Book: Low-FODMAP Recipe Book
References cited in this guide
- Pimentel M, Saad RJ, Long MD, Rao SSC. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. Am J Gastroenterol. 2020;115(2):165-178. PubMed
- Rezaie A, Pimentel M, Rao SS. How to Test and Treat Small Intestinal Bacterial Overgrowth: An Evidence-Based Approach. AGA Clinical Practice Update. Gastroenterology. 2020;159(4):1526-1532. PubMed
- Monash University. 3-Step FODMAP Diet. Monash FODMAP. PDF
- Monash University. About FODMAP and IBS: Frequently Asked Questions. Monash FODMAP. Web
Last updated: March 2026 Author: Beiker Guillen Next review: September 2026
Disclaimer: This information is for educational purposes only and does not replace professional medical consultation. Always consult a specialist physician before making decisions about your health or starting any therapeutic diet.
Important editorial note
This information is for educational purposes only and does not replace individualized professional advice. Always discuss decisions about your health with a qualified professional.
Sources and references
These references guide how this piece is written and updated. They do not replace individual clinical assessment.
Reference1
ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth (2020)Guía clínica del American College of Gastroenterology para diagnóstico y tratamiento.
Reference2
AGA Clinical Practice Update on Small Intestinal Bacterial Overgrowth (2020)Actualización de buenas prácticas con énfasis en límites diagnósticos y manejo clínico.
Reference3
Monash University: 3-Step FODMAP DietResumen oficial del enfoque por fases de la dieta low-FODMAP.
Reference4
Monash FODMAP FAQsContexto práctico sobre reintroducción, tolerancias y uso correcto de la dieta.
Beiker Guillen
Founder of Sibo Wise
I'm not a health professional — I'm a software developer. I started Sibo Wise when my sister was diagnosed with SIBO and I saw how hard it was to find clear, trustworthy information. My role here is research and organization: I gather what serious medical sources say —clinical guidelines from the ACG and AGA, Monash University materials, and PubMed-indexed studies— and cross-check every claim against its original source before publishing.
This content does not replace professional medical advice. If you have any concerns about your health, consult a qualified gastroenterologist or dietitian.